Football has long sold a contradiction: elite strength, elite conditioning, elite survival. But beneath that picture, a much darker pattern has kept surfacing. Former NFL players, despite lower death rates overall, are dying from neurodegenerative diseases far more often than expected.
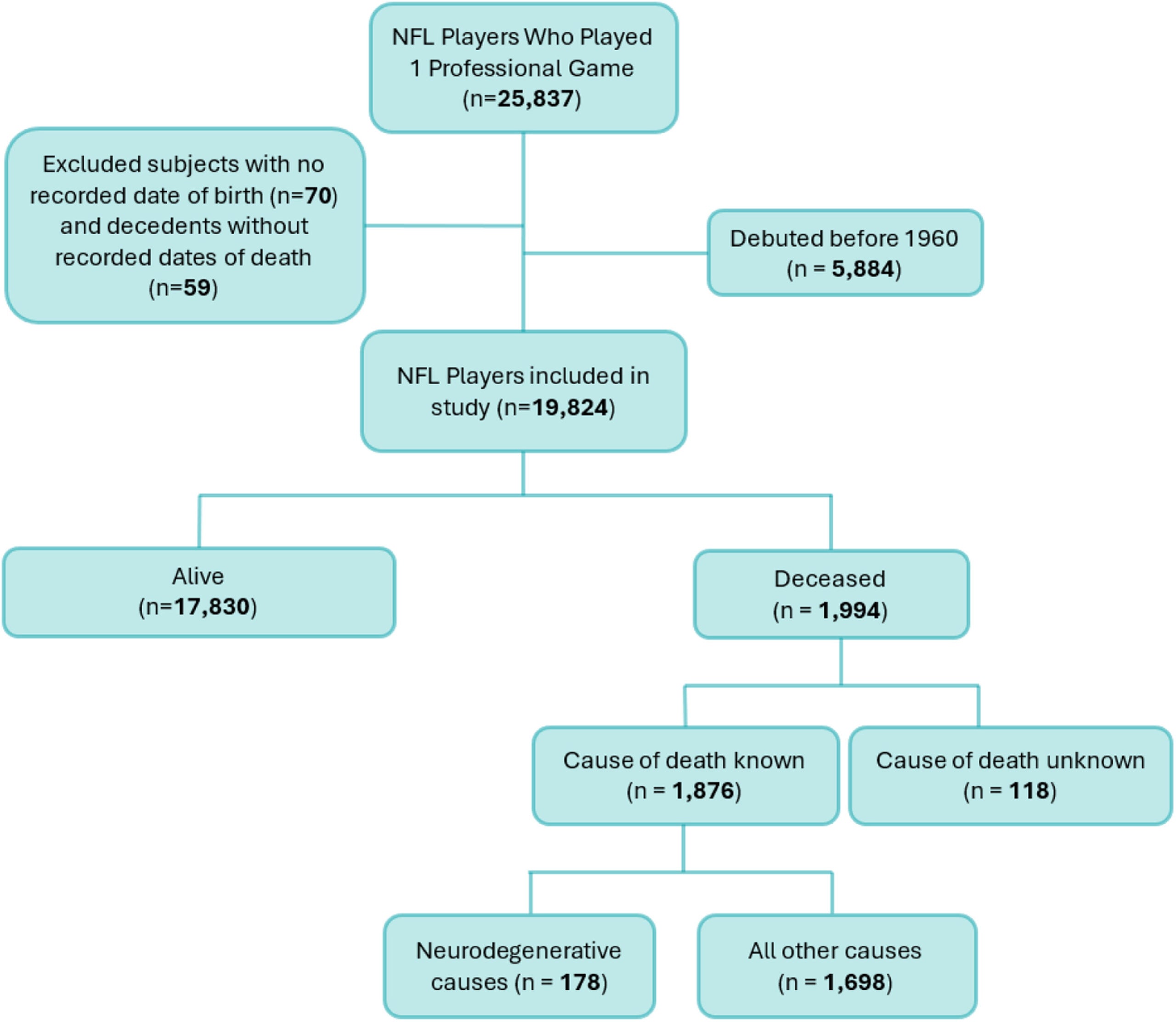
That is the central finding of a large cohort study from Mass General Brigham, Boston University, and the Concussion & CTE Foundation, published in eClinicalMedicine. The analysis followed 19,824 players who appeared in at least one NFL regular-season or postseason game between 1960 and 2019 and tracked deaths through 2023.
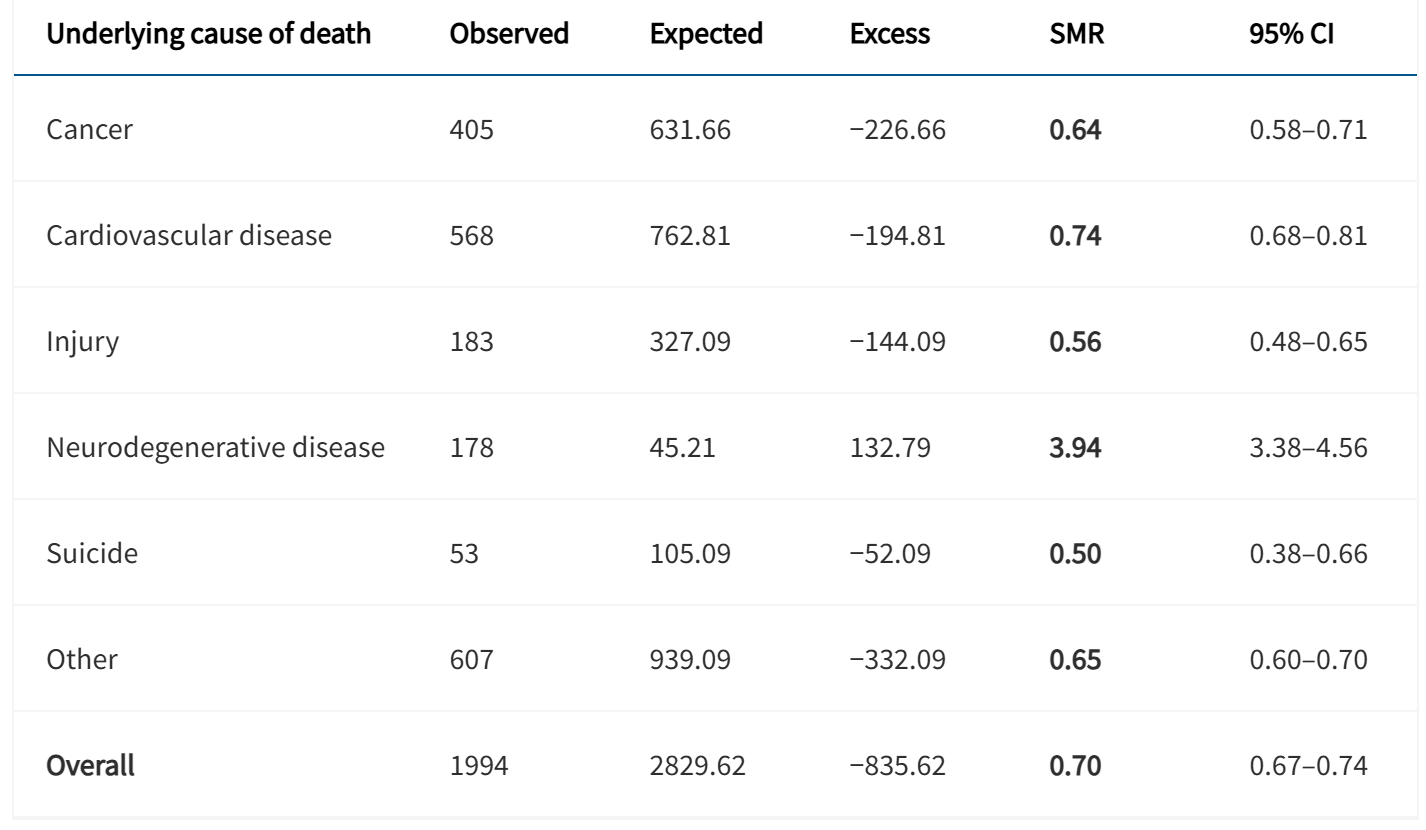
The broad result was unusual and stark at the same time. NFL players had lower mortality than the general population from cancer, cardiovascular disease, injury, suicide, and death overall. Yet their mortality from neurodegenerative disease was nearly four times higher.
“This is the clearest population-level evidence we have ever had that NFL players are dying due to neurodegenerative disease at real and measurably higher rates,” said co-senior author Daniel Daneshvar, chair of Physical Medicine and Rehabilitation at Mass General Brigham and Harvard Medical School and director of the HealthSpan Lab.
He added that across “every official cause of death,” the pattern held: “NFL players are dying of dementia and Parkinson’s disease three to four times more often than they should.”
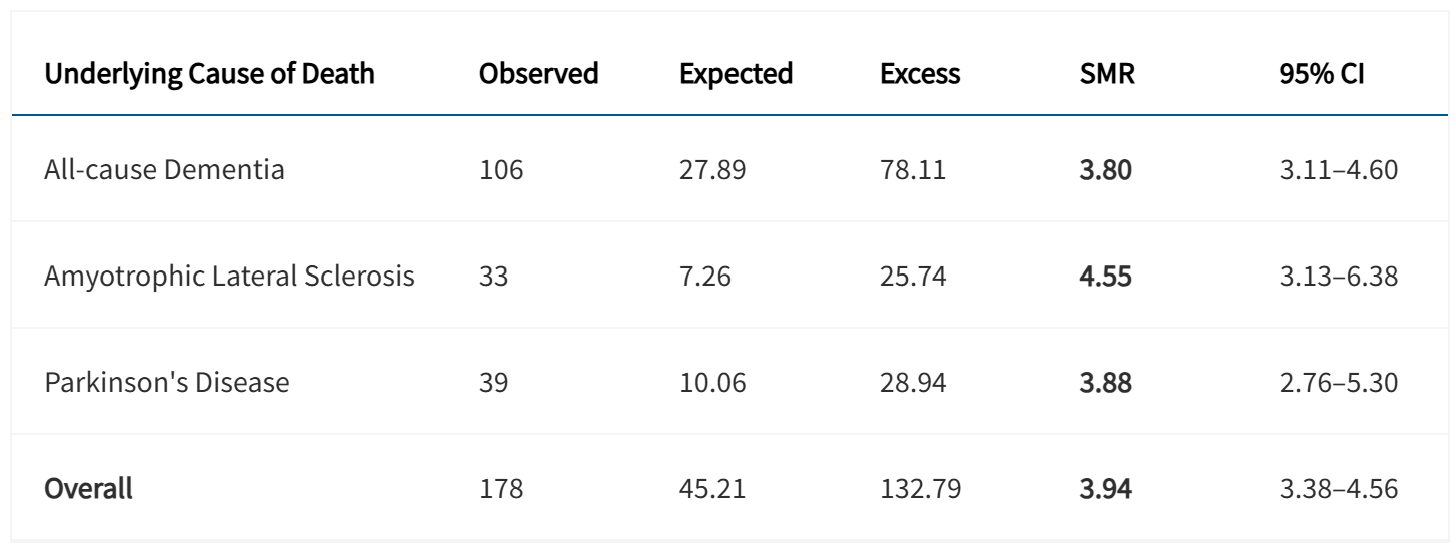
Among 1,994 deaths in the cohort, 178 were attributed to neurodegenerative disease. That included 106 deaths from all-cause dementia, 33 from amyotrophic lateral sclerosis, or ALS, and 39 from Parkinson’s disease.
Compared with the general population after standardizing for age, sex, race, and calendar year, the players’ all-cause mortality was 30 percent lower. Cancer mortality was 36 percent lower. Cardiovascular mortality was 26 percent lower. Suicide mortality was cut in half.
Neurodegenerative mortality moved in the opposite direction. The study found a standardized mortality ratio of 3.94 for neurodegenerative disease overall. Dementia mortality was 3.80 times higher than expected. Parkinson’s disease mortality was 3.88 times higher. ALS mortality was 4.55 times higher.
That split, lower mortality in most major categories but sharply elevated mortality from brain disease, is one reason the findings stand out.
“This is a population that is generally healthier yet still dying of brain disease at higher rates,” the authors wrote.
Jesse Mez, a study co-senior author and associate director of the Boston University Alzheimer’s Disease Research Center and co-director of clinical research at the BU CTE Center, put the size of the effect in plain terms.
“A fourfold increase in dementia rates from a presumed environmental cause is immense, and brain bank studies indicate that CTE is the primary explanation,” Mez said.
The study also found signs of a dose-response pattern. Players whose careers lasted five or more seasons had significantly higher neurodegenerative mortality than those who played one to four seasons.
For the longer-career group, neurodegenerative mortality was 5.27 times higher than expected, compared with 2.21 times higher for shorter-career players. Their dementia mortality was nearly doubled relative to the shorter-career group, and their Parkinson’s mortality was more than doubled.
Players in speed positions, defined here as everyone except offensive and defensive linemen, also faced higher risks in some categories. Speed players had a 67 percent higher neurodegenerative mortality rate than non-speed players and about double the dementia mortality.
The age findings were even more striking. Players who died before age 60 had a 12.43-fold higher neurodegenerative mortality rate than expected for the general population. In that under-60 group, ALS mortality was more than 15 times higher. Additional analysis found that players younger than 50 had a 41.7-fold higher ALS mortality risk than players 50 and older.
The numbers were smaller in those age groups, and the authors cautioned that some early-onset findings could shift with even modest changes in case counts. Still, the pattern suggests that for some players, these diseases are not only more common but may also appear earlier.
To explain why NFL players can live longer overall while still showing much higher neurodegenerative mortality, the researchers proposed what they call the Selection Through Athletic Resilience Survivor, or STARS, effect.
The idea is that people who make it to the NFL are not a random slice of the public. They are more likely to have exceptional physical ability, resilience, self-discipline, and access to training and medical care. They may also be less likely to smoke or carry serious illnesses into adulthood. Those advantages can push overall mortality down.
That makes the elevated brain disease rates more notable, not less.
The team tested whether this longer survival might partly inflate neurodegenerative death rates simply because players live long enough to reach the ages when such diseases become more common. A cause-specific hazard simulation suggested that competing risks could explain only part of the increase. After accounting for that, the residual neurodegenerative mortality rate was still about three times higher than expected.
Even under an extreme model that assumed zero mortality from all competing causes, the excess remained statistically significant.
In other words, the pattern did not disappear when the survival advantage was taken into account.
The researchers also reported some subgroup differences that add complexity. Non-White players had higher ALS mortality than White players, though there were no racial differences for overall neurodegenerative mortality, dementia, or Parkinson’s disease. The study notes that the mortality software used only White and non-White categories, limiting more detailed racial analysis.
The work is large and unusually comprehensive. It includes every player in the eligible era who appeared in at least one NFL game and uses National Death Index records rather than relying on brain donation, symptom reports from family members, or selected case series.
That design addresses some criticisms that have surrounded past research on repetitive head impacts and neurodegenerative disease, especially concerns about selection bias in brain banks and the tendency to focus on symptomatic players.
Still, the study has limits. Death certificates can misclassify neurodegenerative disease, which may lead to undercounting. The analysis used only the underlying cause of death, not contributing causes. It could not determine when symptoms began, when diagnoses were made, or how many former players had chronic traumatic encephalopathy, which is often not recorded on death certificates. The authors also could not fully adjust for factors such as genetics, military service, substance use, socioeconomic status, or other medical conditions.
The study applies only to men and may not generalize to the broader football population.
The findings strengthen the case that former NFL players should be treated as a group with elevated risk for neurodegenerative disease, even when they appear healthier than average in other ways. That has consequences for screening, counseling, long-term care planning, and public policy around repetitive head impacts.
The authors argue that prevention cannot stop at concussion protocols alone. Efforts should also focus on reducing cumulative head-impact exposure over the course of football careers and addressing modifiable midlife risk factors that can worsen later brain health, including hypertension, obesity, diabetes, high cholesterol, and atherosclerosis. They also point to the value of regular physical activity, mental health treatment, and strong social relationships across the lifespan.
For the broader public, the study adds weight to a debate that has often been clouded by small samples, limited follow-up, and arguments over bias. This time, the signal is harder to dismiss. The players in this study were, in many ways, healthier than average. Yet when it came to dementia, Parkinson’s disease, and ALS, they died at rates the general population did not.
Former NFL players who are concerned about their brain health or neurodegenerative disease risk are encouraged to seek evaluation from clinicians specializing in neurodegenerative disease.
Many conditions can cause symptoms that resemble neurodegenerative disease, and many of these conditions are treatable. Even when long-term risk cannot be eliminated, identifying and managing modifiable risk factors can help support overall brain health and quality of life.
Players seeking guidance, specialist referrals, or support in managing health concerns are encouraged to utilize available resources, including The Trust Powered by the NFL Players Association (NFLPA), the NFLPA’s Professional Athletes Foundation, and the Concussion & CTE Foundation HelpLine.
Research findings are available online in the journal eClinicalMedicine.
The original story “NFL players 4x more likely to die due to neurodegenerative disease” is published in The Brighter Side of News.
Like these kind of feel good stories? Get The Brighter Side of News’ newsletter.
The post NFL players 4x more likely to die due to neurodegenerative disease appeared first on The Brighter Side of News.


Leave a comment
You must be logged in to post a comment.