Type 2 diabetes may begin leaving clues in the gut long before a diagnosis arrives. In a large Swedish study, people who later developed the disease shared a pattern of bacterial changes years earlier, including one surprise that could reshape how doctors think about risk.
The work followed 4,685 Swedish adults whose stool samples were analyzed with whole-genome shotgun sequencing, a detailed way to map the gut microbiome. Over a median follow-up of 5.3 years, 383 of them developed type 2 diabetes.
That gave researchers a chance to ask a difficult question that shorter, cross-sectional studies often cannot answer: were the microbial changes appearing after diabetes took hold, or before it?
Their answer was not simple, but it was striking. Several bacterial species and metabolic functions in the gut were tied to future diabetes risk, even after the team accounted for a long list of other factors, including diet, lifestyle and baseline fasting glucose in sensitivity analyses.
The study, led by researchers at Chalmers University of Technology as part of the EU project HealthFerm, drew on the Swedish Infrastructure for Medical Population-based Life-course and Environmental Research, or SIMPLER. The participants were older adults, mostly in their 70s, and none were taking type 2 diabetes medication at the start.
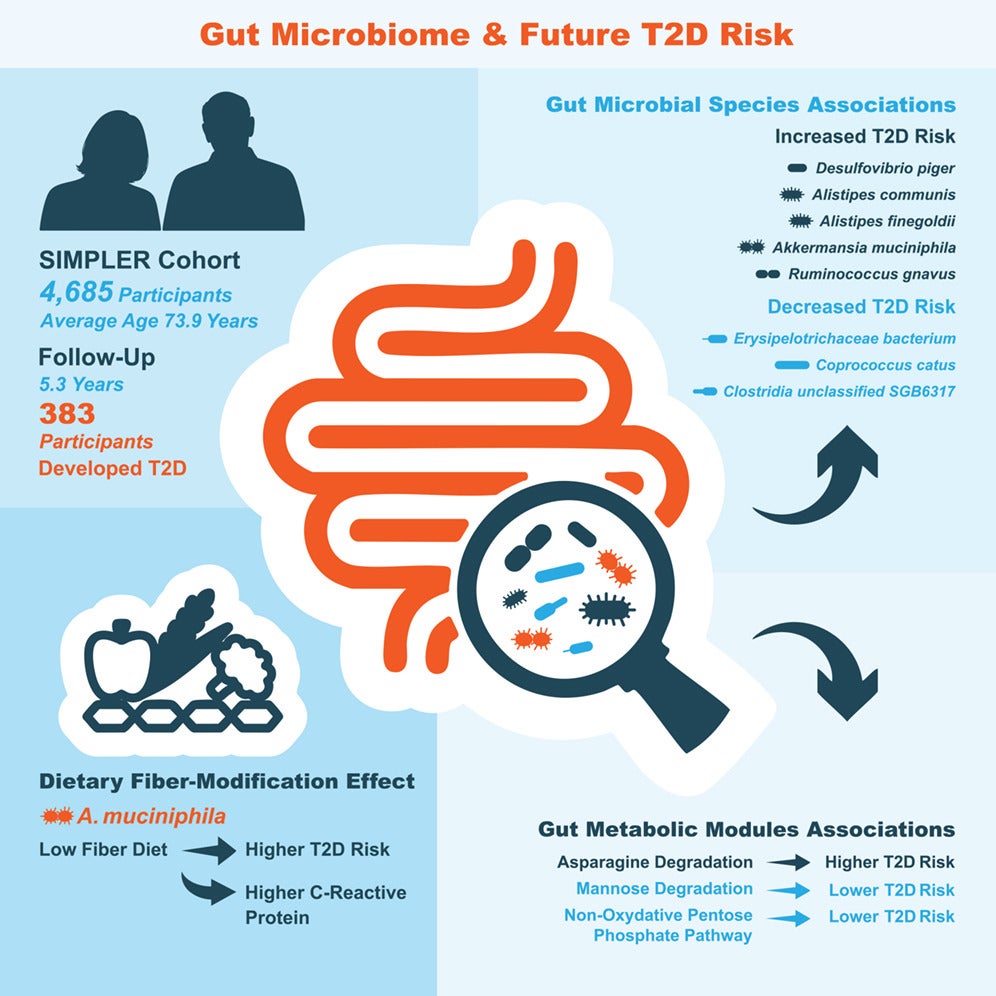
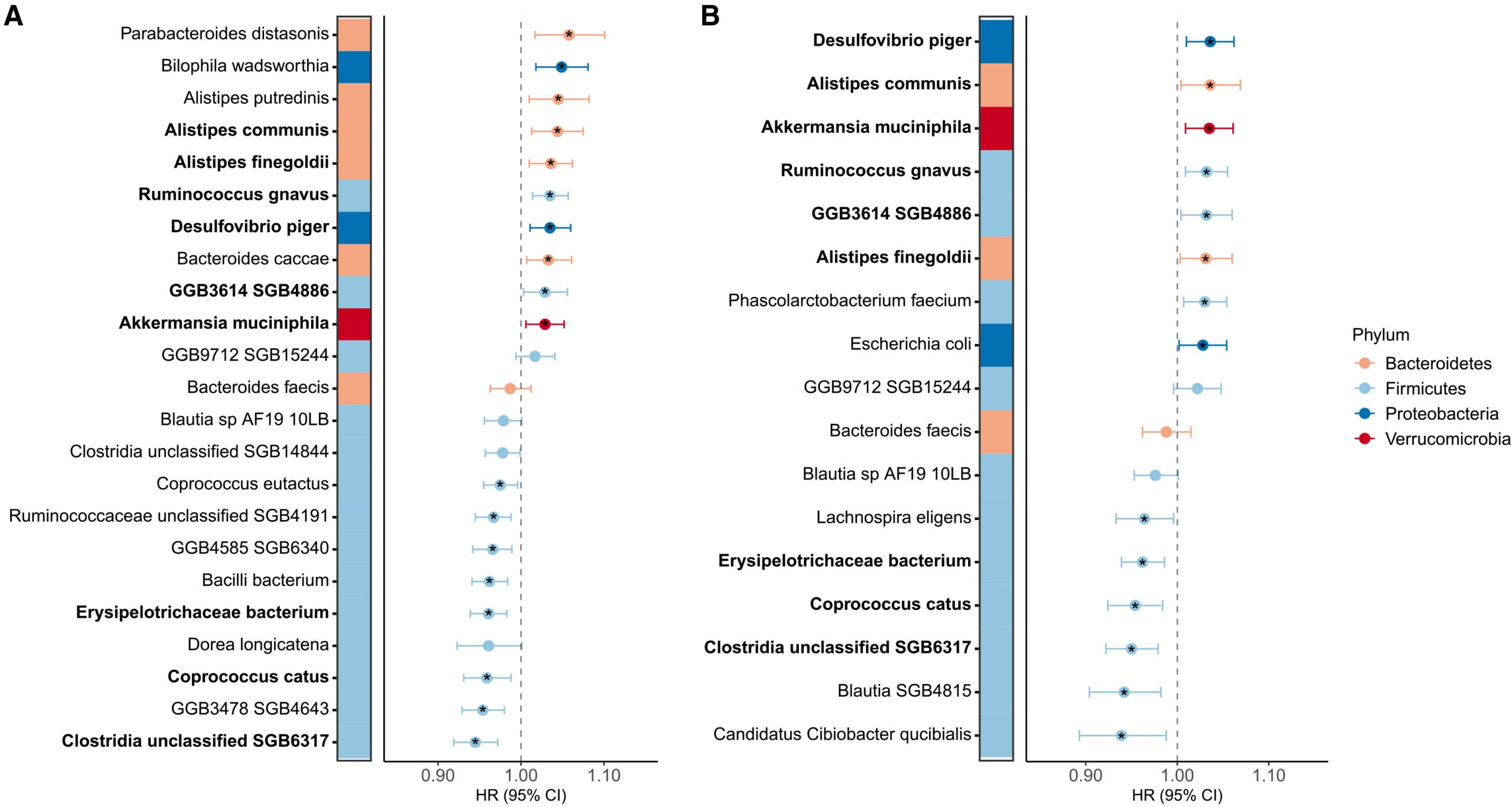
The clearest species-level signal involved nine bacteria that held up across the study’s main analyses. Six were linked to higher future risk, while three were linked to lower risk.
Among the risk-linked microbes were Desulfovibrio piger, Alistipes communis, Akkermansia muciniphila, Ruminococcus gnavus, Alistipes finegoldii and one still-unnamed species-level genome bin. Three others, including Coprococcus catus, an unclassified Erysipelotrichaceae bacterium and an unclassified Clostridia species, were tied to lower risk.
The research also pointed to the gut microbiome’s functional potential, not just which microbes were present. One metabolic module involved in asparagine degradation was associated with higher risk. Two others, tied to mannose degradation and the non-oxidative branch of the pentose phosphate pathway, were associated with lower risk.
Those patterns suggest the story is not only about which microbes inhabit the gut, but also what chemical work they are equipped to do there.
One of the most surprising findings centered on Akkermansia muciniphila, a bacterium often described as beneficial for cardiometabolic health.
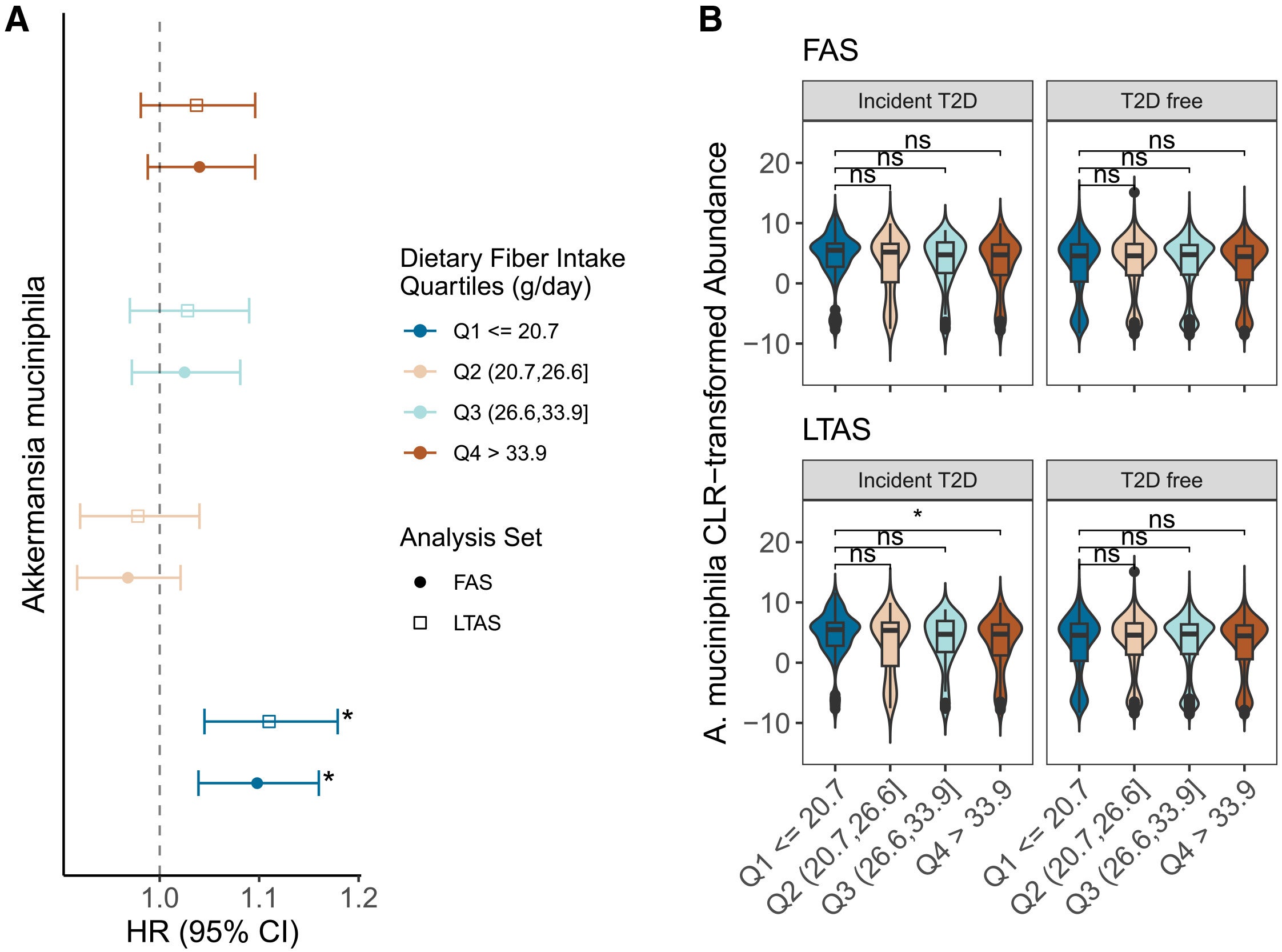
In this study, higher levels of A. muciniphila were linked to a modestly higher risk of later developing type 2 diabetes. Meanwhile, in the main analysis set, the hazard ratio was 1.029. In the lag-time analysis, which excluded people who developed diabetes within the first year, it was 1.035.
That result ran against the way this bacterium is usually discussed, but the team found an important clue when they looked at fiber intake.
Among people in the lowest quartile of dietary fiber intake, defined here as 20.7 grams a day or less, the association between A. muciniphila and future diabetes risk was stronger than it was in the highest fiber group. Formal interaction tests did not reach statistical significance, but the pattern was consistent enough to get the researchers’ attention.
Gaël Toubon, a postdoctoral researcher in food science at Chalmers and one of the study’s authors, said the finding points to a more conditional role for the microbe than its reputation suggests.
“Under favourable conditions, this bacterium feeds on the fibre we get from our diet. But when our fibre intake is too low, it instead starts to break down the gut’s protective mucus layer. This can lead to other bacteria coming into contact with the intestinal lining, causing inflammation and other metabolic disruptions linked to insulin resistance and type 2 diabetes,” he said.
The study also found that among participants who later developed diabetes and had C-reactive protein data available, higher A. muciniphila under low-fiber conditions was associated with higher odds of elevated inflammation, while the pattern flipped under high-fiber conditions.
Other microbes in the risk group fit more comfortably with earlier concerns about inflammation and metabolic dysfunction.
Ruminococcus gnavus, for example, has already been linked in earlier work to metabolic disorders. Here, it again tracked with higher future diabetes risk. Desulfovibrio piger, a sulfate-reducing bacterium, also pointed upward. The paper notes that such organisms may affect the gut barrier, inflammation and hormone signaling in ways relevant to insulin resistance.
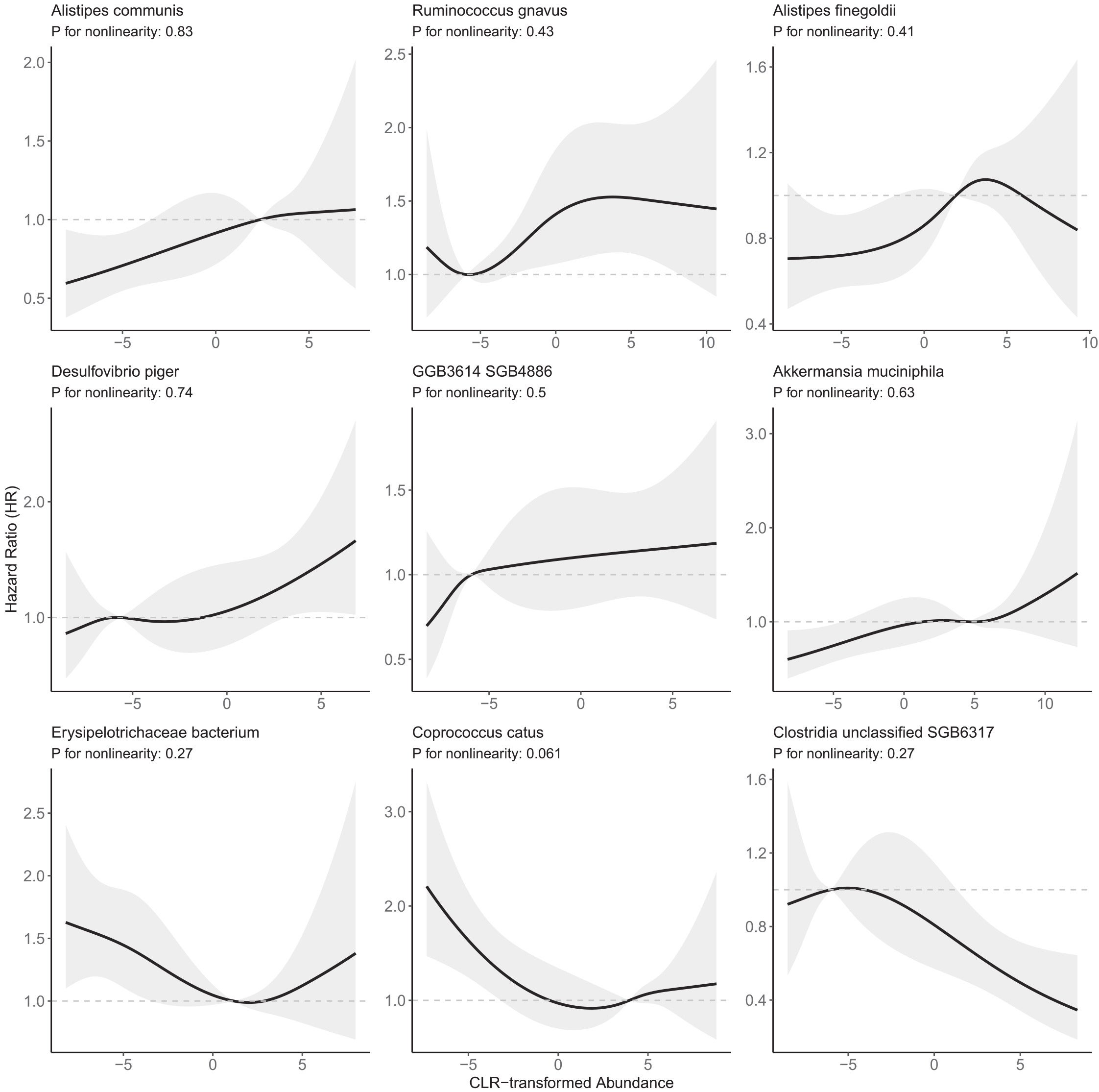
Coprococcus catus stood out on the other side of the ledger. Lower levels were linked to higher risk, but mainly when the bacterium was present at very low abundance. Above that low tail, the added benefit seemed to level off. That matters because C. catus is associated with butyrate production, and butyrate has long been viewed as helpful for gut barrier function and glucose regulation.
The broader message is that the gut microbiome may not act like a simple list of “good” and “bad” bacteria. Context, abundance and diet all appear to matter.
That complexity may help explain why past microbiome research has often produced inconsistent results. Many earlier studies were cross-sectional, meaning they could show association but not timing. Drug use, especially metformin, can also alter the microbiome and blur cause and effect. By focusing on people who were medication-naive at baseline and then tracking who developed diabetes years later, this study tried to reduce some of that confusion.
The study has clear strengths. It used shotgun metagenomics rather than the lower-resolution 16S rRNA approach used in many earlier microbiome studies. It also included one of the largest prospective cohorts of its kind and used inpatient, outpatient and prescription records to identify incident diabetes.
Still, the findings are not a clinical test yet.
The participants were older Swedish adults, so it is not clear how well the same microbial patterns would apply to younger groups or more diverse populations. Some associations weakened after further adjustment for fasting glucose, suggesting that early metabolic changes and microbial shifts may sometimes travel together. The authors also say the work needs replication in other large cohorts.
Rikard Landberg, professor at the Department of Life Sciences at Chalmers and lead author of the study, said the findings support current dietary advice but do not yet justify personalized prescriptions based on a stool sample.
“We cannot yet give that kind of dietary advice, but, at a general level, the study’s findings support current recommendations to eat foods rich in fibre from fruit, vegetables, legumes and wholegrains. Our results emphasise the importance of studying the gut microbiome together with other lifestyle factors, as together they may influence the risk of developing type 2 diabetes,” he said.
The most immediate value of the work is not treatment, but earlier warning. Today, type 2 diabetes risk is often estimated using factors such as obesity, family history and blood sugar. This study suggests stool-based microbiome markers could one day add another layer, helping identify people who appear healthy now but are already moving toward disease.
That possibility is still preliminary, and the authors are careful about that. But if the findings hold up, the gut microbiome may become more than a passive readout.
Because it can change with diet and lifestyle, it could become part of future prevention strategies aimed at delaying or avoiding type 2 diabetes before symptoms begin.
Research findings are available online in the journal Cell Reports Medicine.
The original story “Gut microbes linked to type 2 diabetes years before diagnosis” is published in The Brighter Side of News.
Like these kind of feel good stories? Get The Brighter Side of News’ newsletter.
The post Gut microbes linked to type 2 diabetes years before diagnosis appeared first on The Brighter Side of News.


Leave a comment
You must be logged in to post a comment.