Weight-loss drugs built around the hormone GLP-1 have changed what obesity treatment can look like, but the headline numbers only tell part of the story. In a large real-world analysis, some patients lost little weight, while others shed more than a quarter of their body weight.
That spread matters because it shows just how uneven the response can be, even with medicines that have quickly become some of the most talked-about drugs in the country.
Researchers led by Venky Soundararajan analyzed de-identified electronic health records from academic medical centers in the United States, focusing on patients treated with tirzepatide and semaglutide. After matching the two groups by key baseline characteristics, the team compared 10,339 tirzepatide-treated patients with 10,339 semaglutide-treated patients.
Over two years of follow-up, tirzepatide was linked to greater weight loss overall. Patients taking tirzepatide reached a mean maximum reduction of 14.7% of body weight, or 16.0 kilograms, compared with 10.8%, or 11.6 kilograms, for semaglutide.
The gap widened at higher thresholds. In the matched cohorts, 90% of tirzepatide patients achieved at least 5% weight loss at some point, compared with 82% of semaglutide patients. At least 10% weight loss was reached by 68% of tirzepatide patients and 47% of semaglutide patients. For losses of at least 15%, the figures were 43% and 22%.
The upper end of the distribution stood out even more. Maximal reductions of at least 20% were seen in 26% of tirzepatide-treated patients, versus 12% of semaglutide-treated patients. Losses of at least 25% were observed in 14% of tirzepatide patients and 5% of semaglutide patients.
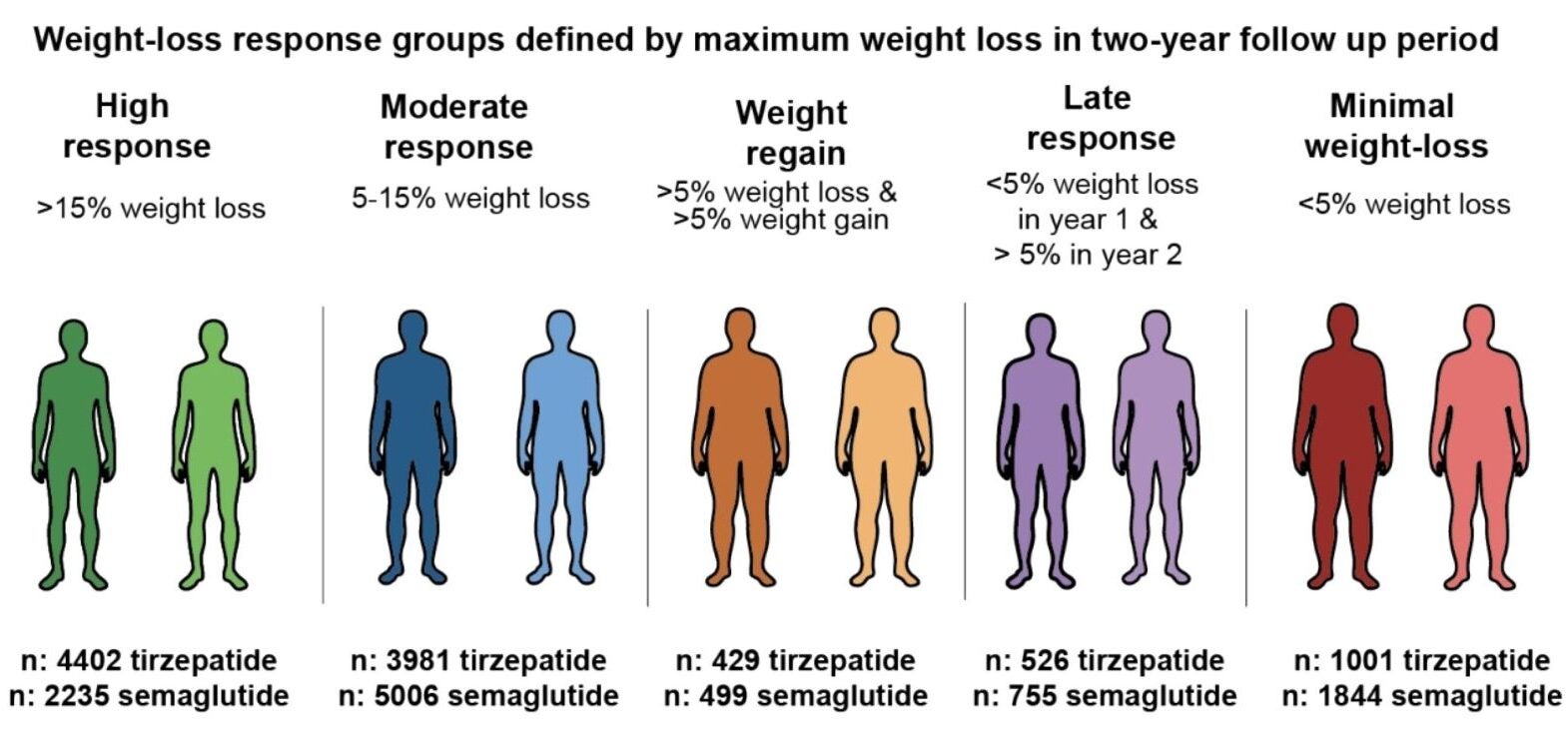
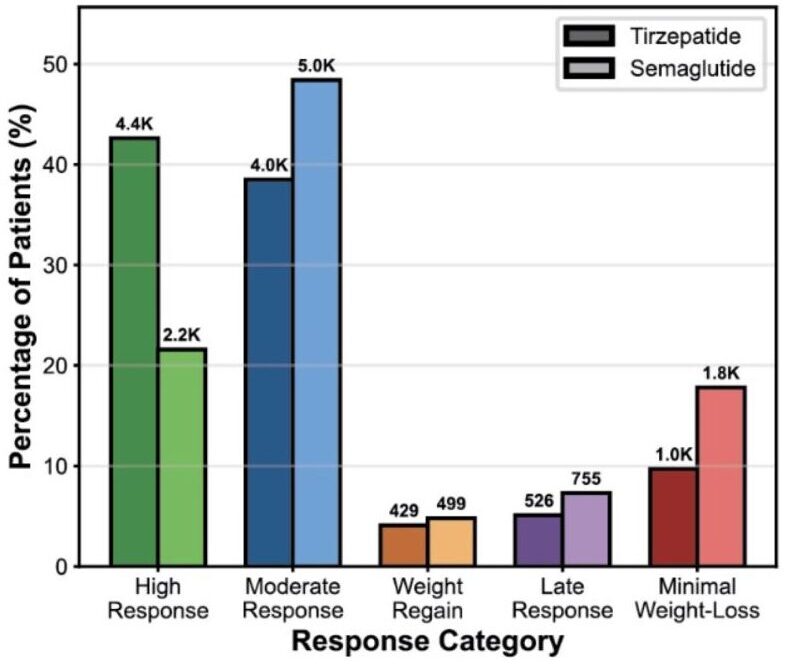
The authors grouped patients into five response patterns: high response, moderate response, late response, weight regain, and minimal weight loss. High responders were defined as people who lost more than 15% of their body weight during the study period. Minimal responders lost less than 5%.
Tirzepatide produced nearly twice as many high responders as semaglutide. It also showed steeper early weight loss. In the high-response group, the mean monthly rate of weight loss during the first six months was 2.54% for tirzepatide and 2.18% for semaglutide.
Those numbers help explain why average outcomes can be misleading. A single mean can flatten a strikingly uneven landscape, where some patients respond strongly and others barely respond at all.
The analysis also found the same demographic pattern across both drugs. White patients were more represented in the high-response group than in the minimal-response group. Black and Hispanic patients were more represented in the minimal weight-loss group than in the high-response group.
For tirzepatide, White patients accounted for 91.2% of the high-response group and 79.8% of the minimal-response group. For semaglutide, the figures were 91.2% and 79.1%.
Black patients showed the opposite pattern. In tirzepatide users, they represented 10.9% of the minimal-response group and 6.0% of the high-response group. In semaglutide users, they made up 10.6% of minimal responders and 5.8% of high responders. Hispanic patients followed a similar trend.
Sex differences appeared too. Women were more represented in the high-response group than in the minimal-response group for both treatments. Among tirzepatide users, females accounted for 74.9% of high responders and 59.2% of minimal responders. Among semaglutide users, the figures were 80.3% and 58.5%.
The authors say the reasons for those patterns are unknown. Their data cannot determine whether the differences reflect biology, access to care, treatment persistence, dose escalation, social conditions, or other factors not captured in the analysis.
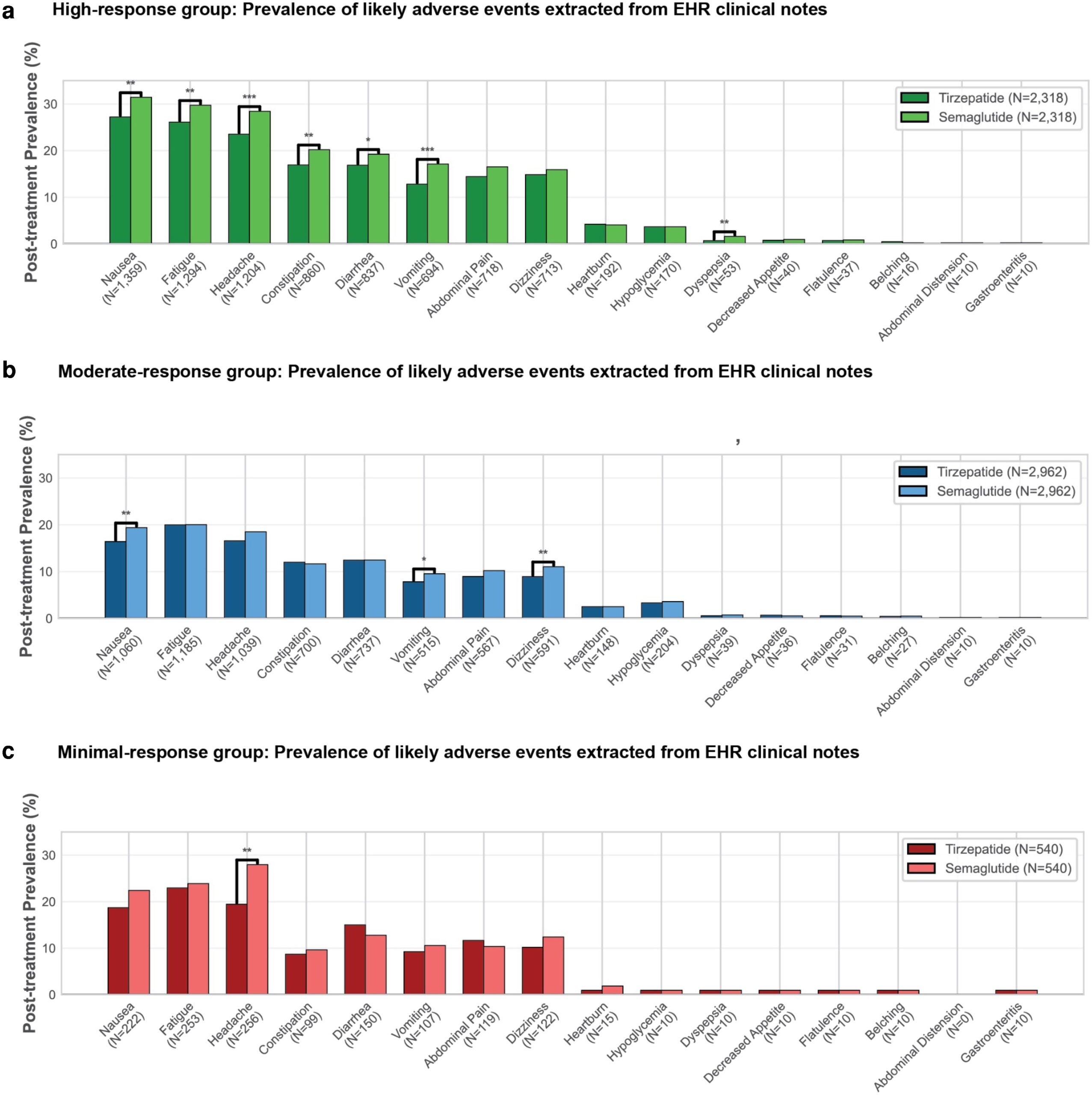
The team also examined 16 commonly reported adverse events using unstructured clinical notes processed through an AI-based information extraction system. In the high-response group, tirzepatide was linked to lower posttreatment prevalence of several gastrointestinal symptoms than semaglutide.
Nausea appeared in 27.2% of tirzepatide-treated high responders and 31.4% of semaglutide-treated high responders. Vomiting was seen in 12.8% versus 17.1%. Constipation occurred in 16.9% versus 20.2%, diarrhea in 16.9% versus 19.2%, and dyspepsia in 0.7% versus 1.6%.
Tirzepatide-treated high responders also had lower prevalence of fatigue, 26.1% versus 29.7%, and headache, 23.5% versus 28.4%. In the moderate-response group, tirzepatide was again associated with lower rates of nausea, vomiting, and dizziness.
That finding is notable because tirzepatide achieved larger and faster weight reductions while also showing lower documented rates of several adverse events. The authors say that separation between effectiveness and tolerability may point to differences between dual incretin agonism and GLP-1-only therapy.
The study drew from a longitudinal database of 23 million patients, then narrowed the sample through prescription, timing, and weight-measurement requirements. Patients with bariatric surgery history were excluded. To improve comparability, the matched analysis excluded patients whose treatment began before January 1, 2023.
Still, the authors are clear about the limits. This was a retrospective observational study, not a randomized trial. Unmeasured confounding could remain, including differences in adherence, documentation, concurrent medications, and social factors such as insurance and access to care. The study also did not assess dose-escalation trajectories in detail, and it grouped different branded formulations of semaglutide and tirzepatide together.
The findings suggest that choosing between these drugs is not just a question of average weight loss. Real-world care may need to pay closer attention to who is responding early, who is not, and who may need a different strategy.
The results also raise a pressing equity question: if some groups are consistently less likely to achieve major weight loss, clinicians and researchers will need to figure out why. For patients, the message is mixed but useful.
These drugs can lead to substantial weight loss, especially with tirzepatide, but the likely result is far from uniform, and response may depend on factors medicine still does not fully understand.
Research findings are available online in the journal PNAS Nexus.
The original story “Tirzepatide vs Semaglutide: Which is more effective in the real world?” is published in The Brighter Side of News.
Like these kind of feel good stories? Get The Brighter Side of News’ newsletter.
The post Tirzepatide vs Semaglutide: Which is more effective in the real world? appeared first on The Brighter Side of News.


Leave a comment
You must be logged in to post a comment.